EHR vs. EMR: What's the Difference and Which Does Your Practice Need?
Author
Fornex Health Team
Published
July 1, 2026
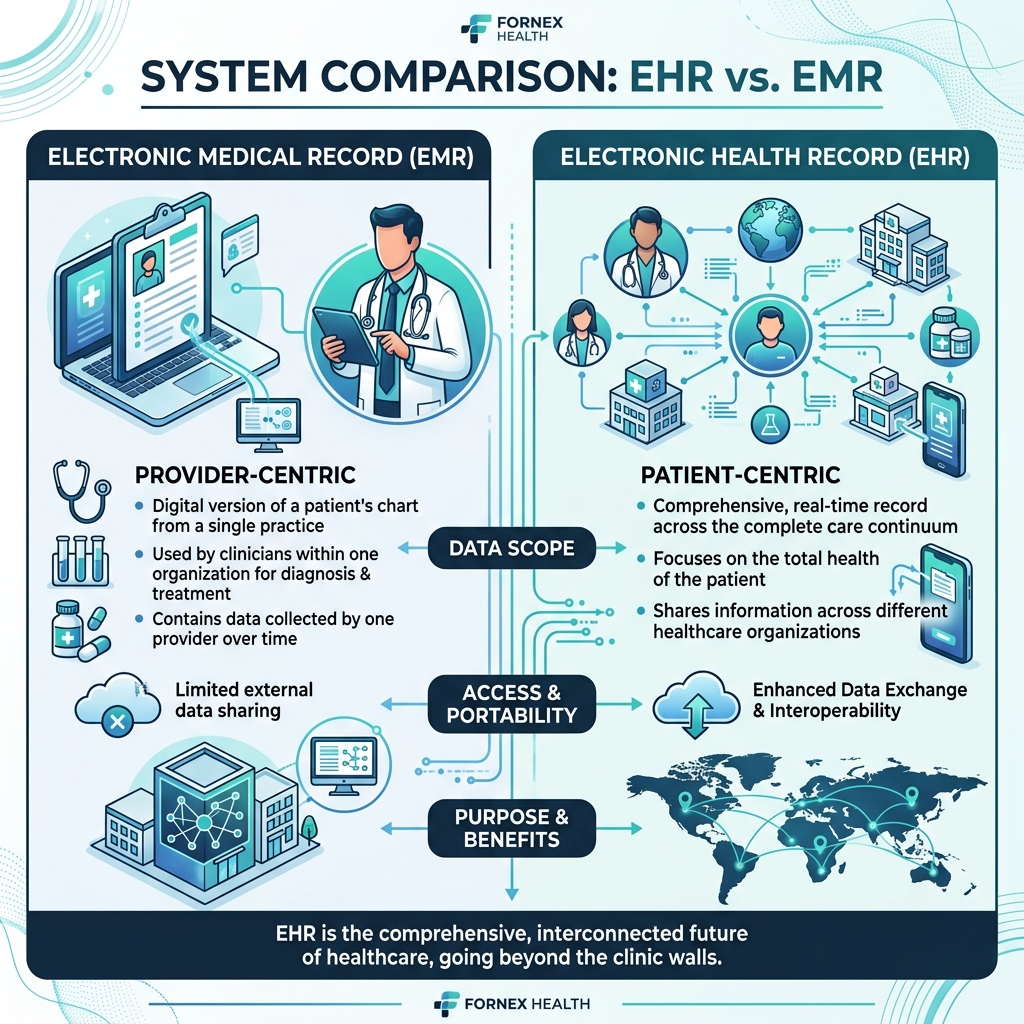
Quick answer: An EMR (Electronic Medical Record) is a digital chart that lives inside one practice—it replaces paper charts but doesn't leave the building. An EHR (Electronic Health Record) is built to travel with the patient: it shares structured data across providers, labs, hospitals, and pharmacies. If your practice operates in isolation and never needs to exchange records, an EMR might technically suffice. If you refer patients out, receive referrals, or need to participate in value-based care or federal incentive programs, you need an EHR, full stop.
The terms get used interchangeably constantly, including by vendors who should know better. Here's what actually separates them, and how to decide which one your organization needs.
EMR: The Digital Version of Your Paper Chart
An EMR is, at its core, a replacement for a paper chart, digitized, searchable, and contained within a single practice. It stores a patient's treatment history, diagnoses, and notes as documented by your team.
The scope of an EMR is intentionally narrow:
- Data stays within your practice.
- Sharing outside the practice typically requires a manual export, printing, faxing, or a PDF download.
- Great for internal documentation and workflow, but highly limited for care coordination.
For a solo practitioner or a small, self-contained clinic that never needs another provider to see a patient's history, an EMR covers the basics.
EHR: Designed to Move with the Patient
An EHR includes everything an EMR does, plus the ability to share that data, in real time, in a structured format, with other providers, labs, pharmacies, and hospitals. This is the single biggest functional difference, and it isn't a minor feature. It changes what the system is fundamentally built to do.
With an EHR:
- Information flows across the care continuum instead of staying siloed in one place.
- Other providers can access relevant, current patient data without a phone call or fax.
- Most modern platforms support structured data exchange standards like HL7 and FHIR, rather than requiring manual export.
Most patients today don't see a single provider for everything. They have a primary care physician, maybe a specialist, maybe an urgent care visit, maybe a hospital stay. An EMR only shows what your practice specifically documented. An EHR shows the fuller picture, which is increasingly what regulators, payers, and patients expect.
The Regulatory Pressure Behind This Distinction
This isn't just a technical nuance, it's increasingly a compliance one. The 21st Century Cures Act requires healthcare data to flow between systems rather than sit locked in individual practice silos. Federal incentive programs like MIPS require EHR-level capabilities, not basic EMR functionality, for reimbursement purposes.
According to CDC data, over 85% of office-based physicians now use electronic records at some level, but "using electronic records" and "meeting current interoperability expectations" are no longer the same bar.
Practically: if you're building new software today, defaulting to EMR-only architecture is choosing to under-build for where the industry and regulations are heading.
Side-by-Side Comparison
| Feature | EMR (Electronic Medical Record) | EHR (Electronic Health Record) |
|---|---|---|
| Scope | Single practice | Across providers and organizations |
| Data Sharing | Manual export (print/fax) | Structured, often real-time exchange |
| Follows the Patient | No | Yes |
| Regulatory Fit | Limited (Cures Act, MIPS) | Built for it |
| Best Fit | Solo/small self-contained practice | Practices that refer, receive referrals, or coordinate care |
So Which One Does Your Practice Actually Need?
A few honest questions to ask yourself:
- Do you ever refer patients to specialists, or receive referrals? If yes, you need EHR-level interoperability, an EMR will create friction every single time.
- Are you part of a larger network, IPA, or value-based care arrangement? Those relationships typically require EHR-grade data exchange as a condition of participation.
- Is your practice growing, adding locations, or planning to? EMRs tend to become a bottleneck the moment a second location or a referral partner enters the picture.
- Do you want to stay eligible for federal incentive programs? Most current programs are built around EHR capabilities, not basic EMR functionality.
If none of those apply, a genuinely small, standalone practice with no referral relationships and no growth plans, an EMR can technically work. In practice, most growing practices outgrow that model quickly, and migrating later is more disruptive than building for interoperability from the start. It's also worth weighing this against what staying on a limited or legacy system actually costs once workarounds and lost referral efficiency are factored in.
Frequently Asked Questions
Can a system be both an EMR and an EHR?
Most modern platforms marketed as "EHR" include EMR-style internal charting as a subset of their functionality. The reverse usually isn't true, a true EMR generally lacks the interoperability layer that defines an EHR.
Is an EHR always more expensive than an EMR?
Not necessarily at the software level, but implementation and integration work (connecting to labs, HIEs, and referral partners) adds cost and complexity that a pure EMR doesn't require. That said, the cost of not having interoperability, manual faxing, duplicate tests, delayed referrals, is a real operating cost that's easy to underestimate.
Does a custom-built system have to choose one or the other?
No, and this is actually where custom development has an edge over off-the-shelf software. You can build internal charting workflows exactly the way your team works while architecting interoperability (HL7/FHIR support) in from the start, rather than being boxed into whatever a vendor decided EMR or EHR should mean.
References
Ready to Build for the Future?
Don't let legacy architecture limit your potential. Connect with us to build a flexible, AI-ready healthcare application.
Talk to Our ExpertsRelated Insights
FHIR Trust Layer
FAST Security: The New FHIR Trust Layer Every Health IT Leader Needs to Understand
Interoperability
Healthcare Interoperability in 2026: The Rules Changed. Most Hospitals Have Not Caught Up.
AI Governance