Agentic AI in Healthcare: What Hospital CTOs Need to Know Before They Pilot Anything
Author
Fornex Health Team
Published
May 6, 2026

Every major health system seems to be announcing an agentic AI pilot right now. Your board wants to know your plan. Your vendors are flooding your inbox. Your peers at other hospitals are posting about it on LinkedIn.
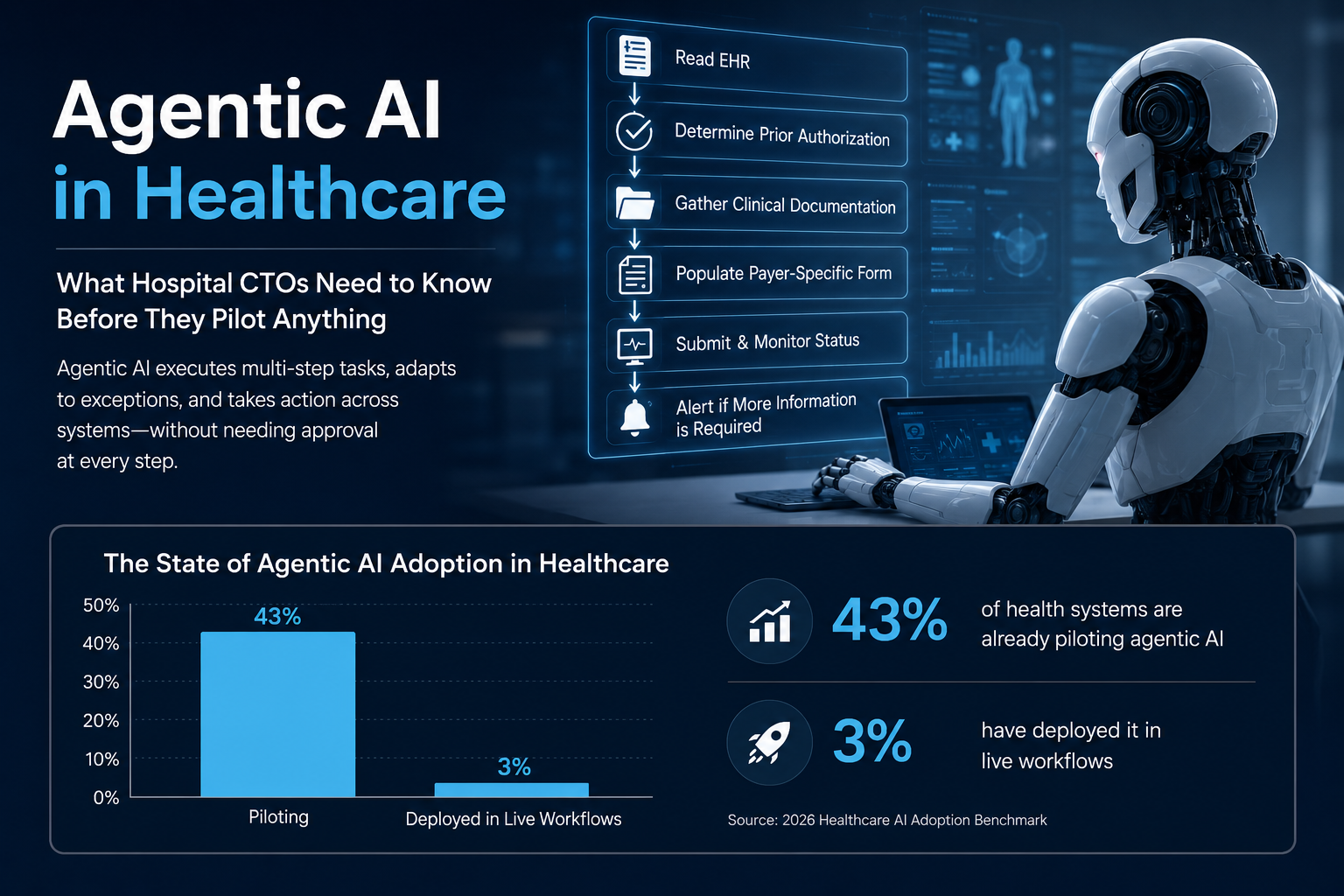
Here is the uncomfortable truth: 43% of health systems are already piloting agentic AI. Only 3% have deployed it in live workflows. That gap is not a coincidence. It is the result of CTOs moving too fast into pilots without first answering some genuinely hard questions.
This is not an argument against moving. Agentic AI is real. The use cases are real. The pressure is real. But the hospitals that come out ahead will be the ones that pilot with clarity, not the ones that pilot fastest.
What "Agentic AI" Actually Means (And Why the Definition Matters)
There is a lot of loose language around this term right now. Vendors are slapping "agentic" onto anything that runs more than one step automatically.
Here is a workable definition. Agentic AI refers to systems that can plan, reason across multiple steps, take actions across different platforms, then adapt when things go sideways without a human approving every move. The difference from traditional automation is that it handles exceptions, not just predictable flows.
A robotic process automation tool follows a script. An agentic system reads the EHR, determines whether prior authorization is needed, pulls the clinical documentation, populates the payer-specific form, submits it, monitors the status, then alerts someone if the payer asks for more information. That entire workflow runs without a coordinator touching it.
That is also what makes it genuinely different from the AI tools most hospitals already have. Ambient scribes, predictive analytics, clinical decision support are all valuable. They assist. Agentic AI executes.

Where It Actually Works Right Now
The use cases getting real traction in 2026 are almost entirely administrative. Prior authorization is the most talked-about. Revenue cycle operations is where the clearest ROI is showing up. Appointment scheduling, discharge coordination, patient portal updates are all areas where agentic systems are replacing hours of manual work.
One health system handling 3.2 million patient interactions per year is saving one minute per call using an agentic system for patient identity verification. That sounds small. It translates to 630 hours of labor per week shifted away from verification toward actual patient assistance.
The clinical side is further behind. Not because the technology cannot do it. It can, in controlled settings. The problem is governance. Before you put an agentic system anywhere near a clinical decision that affects a patient, you need a framework for how it gets authorized, how its actions get audited, how it gets shut down if something goes wrong. Most hospitals do not have that framework yet.
If a vendor is trying to sell you a clinical agentic deployment before you have solved the governance question, slow down.
The Three Questions You Need to Answer Before Your First Pilot
1. What does your data infrastructure actually look like?
Agentic AI depends on clean, accessible, interoperable data. If your EHR, your payer portals, your scheduling systems, your patient engagement tools are all siloed, an agentic system cannot effectively orchestrate across them. You end up with an expensive automation that runs one workflow in one system.
Before you commit to a pilot, map out where your data actually lives. Which systems talk to each other right now via FHIR APIs? Which ones require manual extraction? Which vendor contracts give you API access at all? This work is boring but it determines everything.
2. How will you authorize, monitor, then shut down AI agents?
This is the question that separates hospitals that are ready from hospitals that think they are ready.
Every AI agent that touches protected health information, writes in the chart, initiates a transaction is a new compliance surface. Leading healthcare CIOs are now requiring vendors to answer exactly how their agents are identified, what permissions they operate under, how their actions are logged, then how they get disabled in real time if something goes wrong. If your vendor cannot give you a crisp answer to all four of those questions, that is a red flag. Not a reason to wait for the next version.
3. Who owns the outcomes when the agent makes a mistake?
This one makes people uncomfortable. It should. An agentic system that submits a prior auth with incorrect clinical data, schedules a procedure with the wrong parameters, sends a patient the wrong follow-up instructions are not hypothetical failure modes. They are the failure modes you need to plan for before anything goes live.
Your pilot contract should specify exactly what the accountability structure looks like when the agent errs. Your clinical and legal teams need to be in that conversation before you sign anything.
What a Good Pilot Actually Looks Like
Start with one workflow. Not three. One.
Pick something where the inputs are structured, the outputs are verifiable, the stakes are meaningful but not catastrophic if something goes wrong. Prior authorization processing in a specific service line is a good example. Appointment scheduling for a specific department is another good starting point.
Define success before you start. Not "the system ran." Specific numbers: time saved per transaction, error rate compared to manual processing, volume handled without human escalation. If you cannot define success in advance, you cannot evaluate whether the pilot worked.
Plan a review at 60 days with the same rigor you would apply to any clinical quality initiative. What worked. What failed. What the failure mode was when it failed. What governance gaps the pilot revealed. Then decide whether to expand.
The Honest Reality
Most hospital agentic AI pilots in 2026 will not make it to production. Not because the technology does not work. It does, in the right conditions. They will stall because the data infrastructure was not ready, the governance framework was not in place, the vendor overpromised what the first version could handle.
That does not mean you should wait. It means you should go in with clear eyes. The hospitals building the right foundation right now, clean data pipelines, FHIR-enabled integrations, governance frameworks for AI agents, are the ones that will actually scale these systems in 2027.
The ones chasing the demo are going to spend the next 18 months explaining to their boards why the pilot never became a program. Your job is not to pilot fastest. It is to pilot smart enough that you actually ship something.
Fornex Health helps hospitals evaluate, integrate, then govern healthcare technology. From legacy system modernization to AI-ready infrastructure. If you are working through your agentic AI readiness assessment, talk to our team.
Ready to Pilot Smart?
Don't let your pilot stall. Get an AI readiness assessment and build a foundation that actually scales.
Book Your Readiness Assessment